



ABR Mechanical Stimulation Method
Relaxo Tonic Response – the key principle of the ABR Method
How does ABR Method work for Cerebral Palsy?
• The classic neuromuscular understanding of the brain injury leading to Cerebral Palsy
• The new development in the “fascia” science
• Musculoskeletal duality – competitive neuromuscular & cooperative myofascial systems
• Handling the imbalances – musculoskeletal duality & biomechanical homeostasis
• Musculoskeletal duality & healthy development
• Musculoskeletal duality & cerebral palsy
• Resetting the myofascial system – a major hope for Cerebral Palsy
ABR Method components technical solutions:
ABR Techniques
ABR Mechanical Stimulation Method
In order to understand how the ABR method works, it makes sense to look at it in 2 phases:
1. General intent of the mechanical stimulation to elicit “Relaxo Tonic Response”
2. How does ABR Method work for Cerebral Palsy?
Relaxo Tonic Response
ABR exercise provides mechanical stimulation to the myofascia tissue with the goal of eliciting “Relaxo Tonic Response” from the fascia components of the muscles, joint capsules, bones, and fat. This specific “Relaxo Tonic Response” produces two-fold improvements within the regional organization of connective tissue – releasing the excessively tight and shortened fascia, whilst simultaneously strengthening the weakened and elongated fascia.
The presence of mechanical imbalances are found within the connective tissues and myofascia in any postural or movement disorder. They exist in all scales:
• From the global level of an entire organism to local single anatomical articulations
• From activity states of static, idle and resting to dynamic, accelerative and decelerative activities.
The “Relaxo Tonic response” deals with this universal phenomena of myofascial imbalance in a coherent and mechanically harmonizing way by simultaneously addressing both facets of myofascial imbalance — the excessively strong, mechanically dominant elements and the excessively weak, mechanically deficient elements.
It is well documented in laboratory tests that the connective tissue has the ability to remodel itself into an improved and more energy efficient state following a specific type of mechanical stimulation – the one in which the mechanical impact is uniform and induces the strain to the connective tissue elements within the 1-2% range.
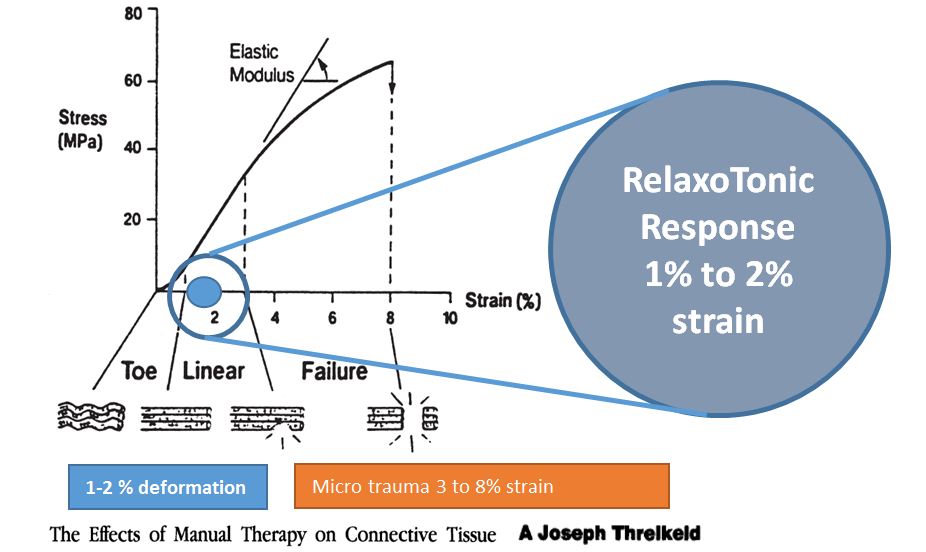
Such a response could be seen as a “reset” of the connective tissue that allows it both to “erase” the existent imbalanced state and “rebuild” itself into a new more balanced and mechanically optimized one.
This is what is needed for the long-term improvement of the musculoskeletal system and locomotor functions in children affected by Cerebral Palsy, because the underlying connective tissue imbalances in their bodies are present at all scales and all the activity states.
As a result, the training protocols based on the active participation and the movements induced by a child himself are most likely to aggravate the global imbalance.
ABR method is a combination of the specific technical solutions delivered via hands-on applications and exercises that provide the mechanical stimulation inducing the “Relaxo Tonic Response” in the different regions of a human body: vertebral column, rib cage, joint capsules, deep muscle attachments etc.
ABR relies on simple yet strict teaching protocols that ensure the delivery of the mechanical stimulations in a precise way that turn the laboratory indications into practical solutions for children affected by Cerebral Palsy.
How does the ABR Method work for Cerebral Palsy?
The classic neuromuscular understanding of the brain injury leading to Cerebral Palsy
The existing theory explains the development of Cerebral Palsy as a disorder of posture and movement following the brain injury, focusing on the fact that a lesion within a central nervous system due to the brain damage disrupts the neuromuscular tone regulation throughout the entire body. Such disruptions and abnormalities of the neuromuscular tone regulation manifest themselves through all sorts of pathological phenomena such as spasticity, rigidity etc. These primary neuromuscular pathologies persist and in turn lead to the gradual structural deterioration of the musculoskeletal system, creating disproportional bone growth, joint deformation and all sorts of the imbalances within the connective tissue,
This explanation naturally concludes that an irreversible brain injury causes the irreversible disruption of the neuromuscular regulation, which then makes the structural imbalances within the musculoskeletal system irreversible as well.
This universally accepted interpretation then points out that there is not much to expect from any direct mechanical impacts aimed at the musculoskeletal system itself, since its structural deterioration and malfunctioning are secondary to the causative brain damage. Naturally this understanding sets very low expectations for the potential benefits that any physical rehabilitation could have – even small improvements in facilitating the basic adaptations of a child to a wheelchair and assisted living are considered to be big enough achievements.
The recent statistical analysis of the therapy outcomes for the children affected by Cerebral Palsy represented by the GMFCS “curves of doom” convincingly confirms this theoretical reasoning. It is shown that whatever condition a child affected by Cerebral Palsy has at two years of age defines what outcome this child is going to have at the age of 18 and older – no matter if any therapies were done or not, and regardless of what kind of therapies were done.
The new development in the “fascia” science
We believe that the recent findings about the architecture, composition and remodelling of the connective tissue – which emerged over the last 10-15 years and became collectively known as the ‘fascia science’ – provide a much broader perspective on how the human musculoskeletal system works and develops compared to the restricted neuromuscular view that dominated the physiology of movements for the entire 20th century.
This broader “fascia” findings open a window for a new understanding of what differences exist in the way the postural and movement functions develop in healthy children and in children affected by Cerebral Palsy. This, in turn, shapes up the new opportunities, showing the new potential avenues for the effective rehabilitation that goes beyond mere adaptation.
Modern “fascia science” points out that our connective tissue manifests itself in many different forms, creating the basic architecture of all the key elements of our musculoskeletal system: bones, muscles, fat, tendons, ligaments, joint capsules etc.
Even more important is the novel understanding that the connective tissue units are not separate entities, but all integrated into a continuous, tensioned network throughout the entire body at all scales – from cellular to organismic – which has a direct built-in mode of mechanical communication called the “small world networks”. This network is also capable of its own “online” direct response to the mechanical stimulations via its own remodelling that reaches as far as the level of modified genetic expression.
Musculoskeletal duality – competitive neuromuscular & cooperative myofascial systems
All those novel findings and scientific understandings allow us to conclude that a human musculoskeletal system is not simply a singular neuromuscular system, but a dual system that combines two rather independent systems for support and movement – the centrally regulated neuromuscular system and autonomously regulated myofascial system.
The mechanical properties of these systems are represented by the biomechanical polarities:
| Neuromuscular system | Myofascial system | |
| 1 | Neuromuscular system is mechanically competitive – being based on the elementary pairs of muscle agonists and antagonists “competing” with each other across the pivotal joints, thus requiring a central control by the nervous system that balances these multiple competing pairs of muscles pulling against each other. | Myofascial system is mechanically cooperative – being integrated into a continuous network that has the built-in properties of rebalancing itself globally to the new steady state regulated by the direct mechanical linkages known as “small world networks”. |
| 2 | The competitive neuromuscular system is compressional in nature – its positional stability depends on the “stacking” of rigid skeletal elements where the tensional elements (ligaments, tendons etc.) are assistive to this primary compressional architecture. | The cooperative myofascial network is tensional in nature – Its positional stability depends on the distributed tensioned state throughout the entire body, where the skeletal elements play the role of tstability and he assistive compressional insertions. |
| 3 | The competitive neuromuscular system has its architecture arranged longitudinally – along the axes and pivots. | The cooperative myofascial network has its architecture arranged radially – volumetrically and curvilinear. |
| 4 | The competitive neuromuscular system is primarily the system designed for acceleration and movement of our body out in the surrounding mechanical environment. | The cooperative myofascial network is primarily the system designed for stability in idle positions, and for deceleration of dynamic impacts that act onto our bodies from the surrounding mechanical environment (reaction forces). |
| 5 | The neuromuscular system is most engaged during the activity and movement. | The myofascial system is most active through the times of idleness, sleep and relaxation. |
Handling the imbalances – musculoskeletal duality & biomechanical homeostasis
From the perspective of Cerebral Palsy, the most important difference between neuromuscular and myofascial systems on the mechanical level is the way they rebalance themselves.
Our body interacts with the external environment via the mechanical impacts that have significant variability in terms of intensity, directions, angular velocities and accelerations. This creates uneven and imbalanced mechanical loadings on the various elements of our musculoskeletal system.
Biomechanical homeostasis characterizes the ability of our bodies to distribute the uneven and variable mechanical perturbations into a balanced remodelling of our musculoskeletal system through time.
That is where we find the greatest difference between the neuromuscular and myofascial systems.
Our neuromuscular system is inherently unstable and has a mechanically built-in tendency for the emergence, persistence and aggravation of the imbalances. This stems from its mechanically competitive nature of the opposing muscles pulling about pivotal articulations. Therefore this system is critically dependent on the neuromuscular coordination provided by the external controller – the central nervous system. If such neurological coordination is disrupted by the damage to the brain, the neuromuscular system inevitably sets itself into the accumulation of deteriorating imbalances.
On the other hand, our cooperative myofascial tensional network has a continuous, radially laid architecture looped onto itself and hence has a built-in tendency to redistribute and integrate any local imbalances and perturbations within the global context. It has a built-in internal controller of mechanically linked “small world networks” where this tensioned system self-adjusts to a globally balanced state.
Musculoskeletal duality & healthy development
Once we have understood this duality of a human musculoskeletal system, the mechanical nature of the deteriorating posture and movement disorder in Cerebral Palsy can be seen in the new light.
In a healthy developing child, neuromuscular and myofascial systems work in a mutually enhancing fashion. The myofascial system “handles” idle positions and weight transfers, whilst the neuromuscular system generates activity. The neuromuscular system exerts acceleration,; the myofascial system handles deceleration.
This combination works in excellent synergy:
• On one hand, the myofascial system distributes the local loads emerging from the reaction forces globally through its entire self, thus providing our body with a low-cost positional support, which in turn allows the neuromuscular system to generate movements and locomotion in an energy efficient way.
• On the other hand, the activity that emerges from the neuromuscular system then “feeds” the myofascial system mechanically – providing the necessary mechanical stimulation to the connective tissues, guiding the continuous internal remodelling that is necessary for maintaining their healthy tone.
During the sleep/relaxation time, all these accumulated impacts stimulate the healthy repairs, growth and development of the structural elements (connective tissue, muscles, bones etc.) that are the same for both systems within our musculoskeletal complex.
Musculoskeletal duality & cerebral palsy
Unfortunately, in a child affected by Cerebral Palsy, this synergistic relationship between the neuromuscular and myofascial systems does not work so smoothly.
The mechanical balancing within competitive neuromuscular system depends on the proper functioning of the central nervous system as its controller. Due to the brain injury this controller cannot perform the fine balancing of the hundreds of competing muscular pulls within the neuromuscular system.
As a result, right from the start of a child’s development the myofascial system is left alone to do the job of maintaining the mechanical balance and providing the sustainable biomechanical homeostasis within the entire dual musculoskeletal system.
In the beginning of a child’s life it is easier – the superficial skeletal muscles that are the main actors within the neuromuscular system are not developed enough yet so the mechanical re-balancing by the myofascial system works well, at least in idle positions. For this reason the young child affected by Cerebral Palsy, especially when asleep, does not present such an obvious difference from a healthy child.
In the early age, the difference between a child affected by Cerebral Palsy and a healthy one only becomes noticeable when a child switches on his neuromuscular system and starts moving. That explains why the official diagnosis of Cerebral Palsy is not announced until a child reaches 12 to 18 months of age.
However, there are two processes that lead to the increasing imbalances later on in the development of a brain injured child.
First, with age, the relative mechanical contribution of the neuromuscular system increases. As a child matures his superficial muscles – most affected by poor neural control –Increase in their size and pulling strength, creating increasing tendencies for neuromuscular imbalance. Hence the myofascial system has to work against greater distorting challenges then before.
Second, the myofascial system itself undergoes the gradual remodelling as it reacts to the imbalanced neuromuscular pulling from within and repetitive imbalanced loads from the external reaction forces. As a result, preferred loading paths within the connective tissue network strengthen and become more densely “woven”, whilst the areas exposed to only minimal stimulation weaken.
Eventually the global re-distribution of forces within the myofascial system becomes compromised as well. Typically that happens after the age of 5 to 7 (even earlier for more severe cases) and only aggravates further, especially during the growth spurts, which add to the neuromuscular imbalance.
Resetting the myofascial system – a major hope for Cerebral Palsy
In a natural course of events in the development of a child affected by Cerebral Palsy, the re-balancing healthy “efforts” of the myofascial system are not enough to “win the campaign” over the distorted neuromuscular system, which eventually prevails and causes the development of the musculoskeletal distortions and deformities to be particularly rapid during the growth spurts periods.
However, there are important conclusions that we should make once we recognize the dual nature of our musculoskeletal system:
1. The healthy stabilizing contribution of the myofascial system. Without its positive contribution that offsets the neuromuscular imbalance, the outcome of the brain injury would be much worse. This is quite obvious in the cases of severe children – the weaker the myofascial system the more severely a child is affected.
2. This gives a new hope for realizing the improvement potential that kids affected by the brain injury have. The information distribution within the myofascial system belongs to the autonomous nervous system and direct mechanical linkages of the “small world networks” that are not damaged by the brain injury. Hence we step away from the hopelessness that the irreversibility of the brain damage instils into the neuromuscular rehabilitation.
The direct mechanical stimulation of the myofascial system can be done in all cases of Cerebral Palsy, even the most severe ones.
It is inspiring to realize that the myofascial system represents the healthy driving forces in the development of a brain injured child. We should try to make the most of these healthy driving forces.
3. The dual nature of our musculoskeletal system gives us a new set of opportunities and allows us to aim for a new target. Instead of fruitlessly trying to train the neuromuscular system as most of the functional rehabilitation methods do today, it makes a lot more sense to target the myofascial system.
The reasons for this are quite obvious:
• The neuromuscular system after brain injury is a dominant one already. Feeding it further with mechanical stimulation through training only increases this dominance.
• The mechanically competitive neuromuscular system is inherently unstable mechanically since its source of balance is neurological system, which was damaged in the case of Cerebral Palsy. Hence, hoping that one can provide a balanced mechanical stimulation to a system that has a distorted neurological controller is wishful thinking.
On the other hand, it makes perfect sense to remodel the myofascial system it in a more balanced way.
• It is a lot more predictable since the myofascial system relies on the autonomous nervous system, which has not been damaged by the brain injury.
• The mechanically cooperative myofascial system has a built-in capacity for “seeking a mechanical balance” once we manage to reset the remodelling processes in it and maintain the correct mechanical stimulation consistently.
In summary, the new improvement opportunities for the children affected by Cerebral Palsy are in finding the better ways of unlocking to the maximum the healthy potential of the myofascial system as a natural driver of a healthy biomechanical homeostasis.
In order to tap into those healthy reserves, we need to find the technical solutions for resetting the myofascial system whilst providing a consistent source of the external mechanical stimulations that induce its internal remodelling into a healthier, more biomechanically balanced state.
ABR Method components technical solutions:
1. Mechanical stimulation – which employs quasi-static, quasi-isotropic and quasi-spherical movements – ensures uniform compression is being delivered
2. 4 bar kinematic linkage – this ensures greatest efficiency of delivery
3. Stress transfer mediums -- matching with the under-lying myofascia structure, these provide the greatest possible impact.
ABR Techniques

Egg Rolling Technique

Super Soft Ball Rolling Technique

Intense Ball Rolling Technique

Accordion Technique

Weighted Ball Technique

Rock Techniques

Single Hand Technique